What types of cancers does DCA & MR10PDCA work on?
DCA & MR10PDCA work for a variety of cancers. These include human studies/case reports and lab studies (rat and in vitro). The cancer types studied so far are: colon, breast, prostate, ovarian, brain (neuroblastoma and glioblastoma), lung (carcinoid), uterus (cervix and endometrial), lymphoma (non-Hodgkins), and cancer of unknown primary.
PATIENTS PRELIMINARY TREATMENT RESPONSES
Treatment protocol generally consists of MR10PDCA in a 3-week on / 1-week off cycle, which is modified based on side effects (e.g. ranges from 1 to 3 weeks of MR10PDCA followed by a rest period). In children, we sometimes offer continuous MR10PDCA treatments. Typical doses are in the range of 20-25 mg/kg/day DCA & 900 mg cannabis oil for adults and 25-50 mg/kg/day 900 mg cannabis oil for children. For elderly patients or those with complicating factors, we may use less than 20 mg/kg/day and 750 mg cannabis oil. The reason that we favour cyclic MR10PDCA treatment is that it allows us to use higher doses and minimize side effects at the same time by having a period of time where the DCA can be cleared from the body. We believe a dose-response relationship exists with DCA (higher doses = better response), therefore cyclic treatment may provide a higher response rate while preventing the drug from being discontinued due to adverse events. It also allows us to clearly determine which side effects are from DCA and which are due to other causes (like the cancer itself). This can be invaluable in determining if DCA should be stopped, or may be safely continued.
Combination therapy implemented (DCA + 1 or 2 treatment/drugs) as DCA works better in combination with other agents than by itself over a prolonged time period.
All of the patients understand that a positive to DCA treatment is not a guarantee and just like most chemotherapies, the individual response varies. We encourage discussion of treatment options, known side effects, monitoring protocol, and the uncertainty and paucity of knowledge of the long term effects of DCA in cancer treatment.

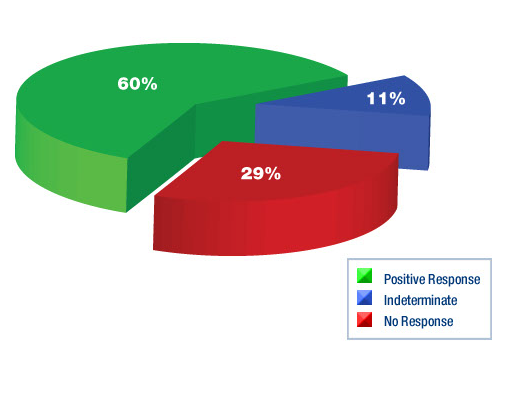
Patient’s evaluation status 4 weeks after start of MR10PDCA treatments
In 179 patients, the following responses were observed specific to the DCA component in MR10PDCA:
106 patients (60%) showed a positive response to DCA. Similar to previous findings, we have divided the positive responses into the following five categories based on the degree of clinical benefit. The categories below are not mutually exclusive since patients may have had a combination of positive responses while on DCA. For example, a patient who had a reduction in tumour size and symptomatic improvement is counted in both categories 1 and 4. For this reason, the numbers below do not add up to 106. This presents an overall picture of the responses to DCA.
Reduction in tumour size/complete tumour regression was seen in 21 patients (12%). We are very excited to report that in 2 patients (1%), we have seen complete remission of metastatic cancer. The other 19 patients (11%) had measurable tumour reduction, which was demonstrated by imaging studies and/or direct tumour measurement.
Reduction in tumour markers was seen in 16 patients (9%). These patients had a reduction in markers such as CEA, CA-125, CA19-9, CA15-3 or AFP. These types of blood markers are typically used to monitor certain cancers such as colon, ovarian, prostate, pancreatic, lung, liver, or breast.
Improvement in blood tests was seen in 12 patients (7%). This included improvements in hemoglobin, liver enzymes, albumin, and other tests indicating reduced tissue damage or reduced cancer activity that could not be explained by other events or medications.
Symptomatic improvement was reported in 52 patients (29%). This included significant pain reduction, relief of bowel obstruction, weight gain, improved appetite and improved energy level. These improvements were sustained for a period of more than 4 weeks, thus making it unlikely to be a result of placebo effect.
Disease stabilization was seen in 61 patients (34%). In these patients, there was no evidence of cancer progression while taking DCA, where progression would otherwise have been expected.
To complete the picture, the following data shows only the best response of each of the 106 patients who had a positive response. We have chosen to define the responses in decreasing level from category 1 to 5 with category 1 (reduction in tumour size) being the best response and category 5 (disease stabilization) being the lowest level of positive response to DCA. The data is categorized as above but here the categories are mutually exclusive with a total of 106 responses. This is unlike the data we have presented previously and therefore is not comparable to our earlier analyses.
Reduction in tumour size was seen in 21 patients (12%), including 2 patients (1%) with complete tumour regression/complete remission. These patients may also have experienced improved blood tests, tumour markers or symptoms, but are not counted in those categories.
Reduction in tumour markers was seen in 14 patients (8%). These patients may also have experienced improved blood tests, improvements in symptoms or disease stabilization, but are not counted in those categories.
Improvement in blood tests was seen in 6 patients (3%). These patients may also have experienced improved symptoms or disease stabilization, but are not counted in those categories.
Symptomatic improvement was reported in 33 patients (18%). These patients may also have experienced disease stabilization, but are not counted in that category.
Disease stabilization was seen in 32 patients (19%). The total of Categories 1-5 is still a 60% positive response rate.
BASED ON OUR OBSERVATIONAL DATA, WE BELIEVE THAT: